Australia,
like much of the western world faces burgeoning numbers of women having caesarean sections along with increasing rates of postpartum haemorrhage, postnatal
depression and other morbidities. There are many who argue for surgical
birth, saying childbearing women are older, fatter and sicker and therefore
require the life-saving operation. Others are critical of the increase. Then there are those who examine the literature and seek the truth of the matter.
Today's blog post is by Dr Kirsten Small, an Obstetrician and Gynaecologist who teaches in the School
of Nursing and Midwifery at Griffith University in Queensland, Australia.
Kirsten has a
research interest in examining the mismatch between the evidence base and what
happens in clinical practice in maternity care.
In line with her research interest, Kirsten provides the following thought provoking lens on a recently published review of the World Health Organisation's target caesarean section rate. Read on, I think you'll find what she has to say fascinating.
Authors Stephen Robson and Caroline DeCosta argue that the “ideal” caesarean
section (CS) rate proposed by the World Health Organization in 1985 is “too low”
(Robson & DeCosta, 2017, p 184).
By selective use of published literature,
they generate a narrative to support this argument, and somewhat obtusely
recommend that “in Australia, we should be aiming to provide CS to all women in
need” (Robson & DeCosta, 2017, p 184). It is difficult to disagree with
this point, but the high Australian CS rate would suggest that we are also
providing CS to women who have no need for it, and who may not desire it.
The
key points of their paper are presented in a summary as Figure 1 below.
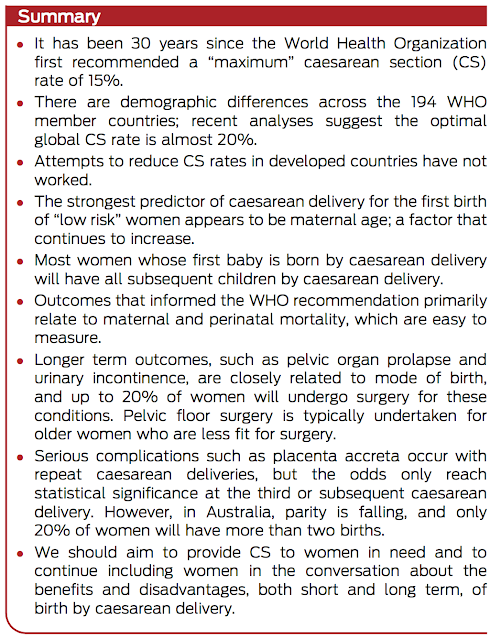 |
| Figure 1: Summary Robson & DeCosta, 2017,
p 181 |
It
is possible however, to use the published literature to create a different narrative, one
that supports the contention that Australia’s CS rate is not appropriate.
An
alternative summary of the evidence is:
- It has been two years since the WHO reaffirmed
its longstanding position that the ideal CS rate is under 20% (Betran, et al.,
2015).
- CS rates, particularly in wealthy
industrialised countries continue to rise, with no evidence of associated
improvement in perinatal outcome (Betran, et al., 2015)
- The strongest predictor of CS birth for the
first infant is birth in a private hospital (Dahlen et al., 2012).
- Women whose first baby is born by CS find it
difficult to access a care provider who will support them to achieve a vaginal
birth in subsequent pregnancies (Toohill, Gamble, & Creedy, 2013).
- Outcomes that interest the patriarchal medical
model typically exclude those that reflect women's experience of their care (Parry, 2008).
- Longer term outcomes for the neonate are
better following vaginal birth rather than CS (Hyde, Mostyn, Modi, & Kemp, 2011).
- Pelvic organ prolapse and incontinence are not
strongly correlated with mode of birth (Bozkurt, Yumru, & Şahin, 2014). Surgical procedures for these conditions are
increasingly safe and carry low risks of complications (Ogah, Cody, &
Rogerson, 2011).
- Serious complications of CS such as placenta
accreta, while rare, are of increasing concern to health care systems, given
the large number of operations performed annually (Cheng, Pelecanos, & Sekar, 2016).
- We should aim to provide all women with
evidence based care that achieves high rates of vaginal birth (Caughey, Cahill, Guise, & Rouse, 2014). All women should be involved in decision
making regarding their birth options, to the extent that they wish to be.
Conclusion: There
are ingrained systemic reasons why the medical model presents CS as the safe,
easy option for women (Bryant, Porter, Tracy, & Sullivan, 2007). The evidence is clear – there is no
population benefit for a CS rate of over 15%. Clinicians should focus on
applying evidence to the care of individual women in order to achieve the best
outcomes for them and for their infants.
References
Betran, A.P., Torloni, M.R., Zhang,
J., Ye, J., Mikolajczyk, R., Deneux-Tharaux, C.,Gülmezoglu, A.M. (2015).
What is the optimal rate of caesarean section at population level? A systematic
review of ecologic studies. Reproductive Health, 12(1), 57–57.
http://doi.org/10.1186/s12978-015-0043-6
Bozkurt, M., Yumru, A. E., & Şahin, L.
(2014). Pelvic floor dysfunction, and effects of pregnancy and mode of delivery
on pelvic floor. Taiwanese Journal of Obstetrics and Gynecology, 53(4),
452–458. http://doi.org/10.1016/j.tjog.2014.08.001
Bryant, J., Porter, M., Tracy, S., &
Sullivan, E. (2007). Caesarean birth: Consumption, safety, order, and good
mothering. Social Science & Medicine, 65(6), 1192–1201.
Caughey, A. B., Cahill, A. G., Guise, J.-M.,
& Rouse, D. J. (2014). Safe prevention of the primary cesarean delivery. American
Journal of Obstetrics and Gynecology, 210(3), 179–193.
http://doi.org/10.1016/j.ajog.2014.01.026
Cheng, H. C., Pelecanos, A., & Sekar, R.
(2016). Review of peripartum hysterectomy rates at a tertiary Australian
hospital. Australian and New Zealand Journal of Obstetrics and Gynaecology,
56(6), 614–618. http://doi.org/10.1111/ajo.12519
Dahlen, H. G., Tracy, S., Tracy, M., Bisits,
A., Brown, C., & Thornton, C. (2012). Rates of obstetric intervention among
low-risk women giving birth in private and public hospitals in NSW: a
population-based descriptive study. BMJ Open, 2(5),
e001723–e001723. http://doi.org/10.1136/bmjopen-2012-001723
Hyde, M. J., Mostyn, A., Modi, N., & Kemp,
P. R. (2011). The health implications of birth by Caesarean section. Biological
Reviews, 87(1), 229–243.
http://doi.org/10.1111/j.1469-185X.2011.00195.x
Ogah, J., Cody, D.J. & Rogerson, L.
(2011). Minimally invasive synthetic suburethral sling operations for stress
urinary incontinence in women: A short version Cochrane review. Neurourology and Urodynamics, 30,
284–291. doi:10.1002/nau.20980.
Parry, D. C. (2008). “We wanted a birth
experience, not a medical experience”: exploring Canadian women's use of
midwifery. Health Care for Women International, 29(8), 784–806.
http://doi.org/10.1080/07399330802269451
Robson, J., & de Costa, M. (2017). Thirty
years of the World Health Organization's target caesarean section rate: time to
move on. The Medical Journal of Australia, 206(4), 181–185.
http://doi.org/10.5694/mja16.00832
Toohill, J., Gamble, J., & Creedy, D. K.
(2013). A critical review of vaginal birth rates after a primary Caesarean in
Queensland hospitals. Australian Health Review, 37(5), 642–7.
http://doi.org/10.1071/AH13044
